Keywords
vaccine hesitancy, maternal vaccines, tetanus toxoid, expectant mothers
This article is included in the Sociology of Vaccines collection.
vaccine hesitancy, maternal vaccines, tetanus toxoid, expectant mothers
We thank the reviewers for their thoughtful and meticulous critique, which has greatly strengthened our manuscript. Their insights prompted several important revisions that have enhanced both the rigor and clarity of our work.
One key correction involved updating our description of the vaccines administered to pregnant women in Kenya. Following the reviewer’s observation, we replaced references to the tetanus toxoid (TT) vaccine with the more accurate tetanus and diphtheria toxoid (Td) vaccine, reflecting the 2019 WHO SAGE recommendation and the near-universal adoption of Td by countries procuring vaccines through UNICEF.
We have removed the citation that alluded that missed opportunities for immunization (MOI) contributes to vaccine hesitancy as it remains unclear how MOI hinders vaccine uptake. To provide a more comprehensive perspective, we expanded the introduction to discuss the influence of male decision-makers on maternal vaccine uptake.
For the methodology, we clarified how expectant mothers were selected for focus group discussions (FGDs), detailed the number of FGDs conducted, and explained the selection for surveying men and women of reproductive age with the assistance of community health extension officers. We elaborated on our qualitative analysis approach and described our handling of missing data. The data collection section was also refined for greater precision.
In the results, we eliminated comparative analyses with other studies to maintain focus on our findings, instead bolstering our interpretations with additional participant quotes. To improve data presentation, we added a table stratifying vaccination knowledge and awareness by sex.
Collectively, these revisions have sharpened the manuscript’s focus, resolved confusing arguments, and reinforced the validity of our conclusions.
See the authors' detailed response to the review by Berhaun Fesshaye
Globally, the World Health Organization (WHO) estimates that in 2019 alone, 2.4 million children died in their first month of life (WHO 2020). Among the causes of these deaths are infectious diseases. Although substantial progress has been made in child survival since 1990, neonatal deaths remain relatively high in sub-Saharan Africa compared to other regions. Children born in sub-Saharan Africa are ten times more likely to die in their first month than their counterparts in high-income countries (WHO 2020). Maternal immunisation can contribute to a significant reduction in neonatal morbidity and mortality. For instance, it is estimated that maternal tetanus vaccine reduces mortality from neonatal tetanus by 94% (Blencowe et al. 2010). Immunization of pregnant women offers a chance to transplacentally transfer protective antibodies to the fetus, conferring protection to the vulnerable infants in the first six months of life when they are exposed but have not developed adequate functional antibody response (Marshall et al. 2016).
Despite the compelling benefits achieved through vaccination, there is a growing concern about vaccine hesitancy. The WHO Strategic Advisory Group of Expert on Immunization defines vaccine hesitancy as a ‘delay in acceptance or refusal of vaccination despite the availability of vaccination services’, which varies across time, place and the vaccine. Vaccine-hesitant individuals may accept all vaccines but remain concerned about vaccines; some may refuse or delay some vaccines but accept others; others may refuse all vaccines (Larson et al. 2014, 2015). In 2019, WHO listed vaccine hesitancy among the top ten public health threats that need attention, a rallying call to governments, public health officials, and advocacy groups to pay attention to this issue. Left unchecked, vaccine hesitancy and misinformation that can spread rapidly through the internet (Cornwall 2020; Enserink 2020) can significantly contribute to a decrease in immunisation rates and hamper the uptake of newly introduced vaccines (Schaetti et al. 2009; Larson, Brocard, and Garnett 2010). For example, in North East Nigeria, vaccine myths, hesitancy, and misinformation that spread within the communities provided significant setbacks to the campaign to eradicate polio (Usman, Bologna, and Stamidis 2019).
Currently recommended vaccines for pregnant women include tetanus toxoid, influenza vaccine and Tdap vaccine (Williams et al. 2019), although countries have different guidelines and can choose which vaccines to administer. The Kenya Expanded Programme on Immunization recommends that expectant women receive tetanus diphtheria (Td) vaccine. However, the Ministry of Health is exploring evidence-based strategies ahead of the anticipation of rolling out the influenza vaccine (McMorrow et al. 2017; Dawa et al. 2019). The success of these vaccines depends on whether mothers decide to use them.
Several factors that contribute to vaccine hesitancy have been reported. These include expectant women’s levels of knowledge and attitude towards the safety and efficacy of the vaccine (Bushar et al. 2017; Eppes et al. 2013) and how the healthcare worker interacts with mothers (Bukenya and Freeman 1991). Literature specifically looking at maternal vaccination in Kenya is sparse. Most studies have focused on coverage and implementation of Antenatal Care (ANC), and on whether ANC services contribute to better neonatal care and assessment of ANC services as a package (Afulani et al. 2019; Arunda, Emmelin, and Asamoah 2017). In this study, we aimed to assess factors contributing to maternal tetanus toxoid vaccine hesitancy within a rural setting of Kilifi County in Kenya.
Other factors that influence motivation for maternal vaccine uptake include the views of the people around the expectant women. It has been shown that husbands and mothers-in-law play a role in the expectant women decision making process during pregnancy including whether to take or not take a vaccine, coupled with the fact of the woman’s limited autonomy within the family setting, especially so within the African context (Johm et al. 2021). In other settings, expectant women seek advice on whether to be vaccinated or not from their female family members such as sisters who already have children, mothers and aunts but less so from their male partners (R. Wilson, Paterson, and Larson 2019).
We obtained scientific and ethical approval from the Pwani University Ethics Review Committee; ERC/PU-STAFF/002/2020. The study got approval from the National Commission for Science Technology and Innovation (NACOSTI) under license number NACOSTI/P/20/6193. The county government Department of Health Services authorised the study to be carried out in Kilifi County.
The study design was cross-sectional, using a mixed methods approach for data collection where both quantitative and qualitative data were collected. We used the qualitative data for cross-validation and corroboration of the findings within the study. Since study activities were conducted during the COVID-19 pandemic, the study team followed the infection control guidelines put in place by the County Department of Health Services to reduce SARS-CoV-2 infections such as social distancing; regular hand washing; use of personal protective equipment to protect oneself and participants; and measuring temperatures of study team before each field visits. Eligible participants gave written consent before participation in the study.
The study was conducted in Kilifi County, located along the Kenyan Coast. In Kenya, the health delivery system is currently a devolved function of the 47 counties. It is organised into six levels but anticipated to transition to four levels: level four, National referral hospitals; level three, county hospitals; level two, primary care facilities (formerly the dispensaries and health centres); and level 1, community hospital (Muinga et al. 2020).
We used convenient sampling for expectant women attending the ANC clinic at select participating health care facilities of Kilifi County Hospital (KCH), Mnarani hospital, and Ngeranya dispensaries. The dispensaries were selected based on the volume of expectant women they receive. We aimed to balance the study population selection to allow us to have a mix of both town settings (Mnarani) and rural settings (Ngerenya). We identified women and men of reproductive age at the community level through the assistance of Community Health Extension Officers, who have good knowledge of their communities and also served as study facilitators. This approach has also been used in other studies (Watson-Jones et al. 2015). The selection of men and women of reproductive age was done at the community level in four different locations/wards (Tezo, Chasimba, Kibarani and Sokoni). The selection of study wards was based on immunisation coverage from Kilifi County’s Kenya Health Information System (KHIS). According to the 2019 KHIS data, the percentage of women who received their first tetanus toxoid vaccine ranged from 6% to 61.2% (lowest to highest) across the 35 administrative wards. We split the percentage of tetanus toxoid vaccine coverage into four quartiles (0-25, 25-50, 50-75 and 75-100) and then selected wards from each quartile as a representative.
To guide the assessment of the factors contributing to the maternal vaccine hesitancy, we adapted WHO’s behavioral and social drivers (BeSD) of vaccination framework ( Figure 1). The BeSD model comprises four key domains of behavioural and social drivers of vaccination which, put together, influence vaccine uptake:
1. Thinking and feeling, which includes the cognitive and emotional responses of people to vaccine-preventable diseases and vaccines;
2. Social processes, which include social norms about vaccination and receiving recommendations to be vaccinated.
3. Motivation, which includes the intention, willingness, and hesitancy of people to get vaccinated; and
4. Practical issues, which include the experiences people have when trying to get vaccinated, including barriers faced, e.g. accessing the clinic or costs of transport to the clinic.
Data collection question guides and questionnaire design were based on quantitative surveys, interview guides and priority indicators corresponding to the BeSD framework’s four domains (Brewer et al. 2017). The questionnaire had a mix of open-ended questions and closed questions on a five-point Likert scale. Senior members of the research team reviewed the questionnaire and question guides and modified them appropriately to fit the local context while retaining the intended meaning. The questions were translated into Kiswahili, a local language for ease of administration. Interview guides were used flexibly to support rich and broader discussion around maternal vaccine hesitancy issues.
Our study used triangulation method to understand factors contributing to maternal vaccine uptake within the rural setting of Kilifi, Kenya. Before data collection the study team underwent training on the overall aims and objectives of the study, the consenting process and the data quality and management processes. We then conducted:
• Focus Group Discussions (FGDs): 10-12 expectant women per group, selected via convenience sampling from high-volume facilities to ensure urban-rural diversity. FGDs (60–90 min) took place during maternal health clinic days. The final sample size of the FGDs was 45.
• Surveys: Administered to 104 selected men and women of reproductive age. We identified women and men of reproductive age at the community level through the assistance of Community Health Extension Officers, who have good knowledge of their communities and also served as study facilitators. This approach has also been used in other studies (Watson-Jones et al. 2015).
• Key Informant (KI) Interviews: Six interviews (30–60 min) with healthcare workers and vaccine managers, conducted at their workplaces.
All FGDs and KIs were audio-recorded (encrypted) and noted by hand. Two researchers (PKK and ROM) conducted face-to-face interviews. Written consent was obtained from all participants. Data collection occurred between September and October 2020.
Quantitative survey data was analysed using STATA version 16. Baseline characteristics of participants including gender, marital status, level of education, and religion are presented as frequencies and percentages. The qualitative data were audio-recorded, transcribed verbatim, and translated into English. We conducted thematic analysis following Braun and Clarke’s (2006) approach, with a particular focus on latent themes. This analytical level moves beyond surface-level content to examine the underlying assumptions, conceptual frameworks, and ideologies shaping participants’ responses (Braun & Clarke 2006, p. 84). Our analysis sought to identify meaningful patterns that could inform our research questions, paying particular attention to the implicit meanings and theoretical constructs embedded in the data. Code reports were generated and analysed by PKK and ROM. Missing data were handled as follows: For qualitative data, participants could opt out of answering any questions. For quantitative data, missing values were included in the analysis and reported as non-responders, as indicated in Table 1 and Figure 2.
The survey respondents were a random sample of 104 adults. Their characteristics and summary are shown in Table 1. Women made up 63 (61%) of the study population, and 80 (77%) of the participants were married. Most participants had primary-level education. The median age was 33 years.
To assess the level of awareness, we asked respondents whether they had ever heard of a vaccine, whether they knew which vaccines expectant women receive and whether they had ever heard of the tetanus toxoid vaccine. Almost all respondents, 98% (102/104), were aware of vaccines, but only 70% (73/104) knew which vaccine women receive when they are expectant, and this level of knowledge was higher in female than males ( Table 2). Interestingly, 93% (97/104) reported knowing the existence of tetanus vaccine.
Expectant mothers reported that the healthcare worker informs them about the vaccine they received, although they don’t interrogate what the vaccine does.
When you are told you are being given the tetanus injection, you know it protects both you and the child concerning tetanus, so we don’t ask questions with regard to its purpose … We are not usually told why we are getting the injection. Expectant Mother FGD4
However, these expectant mothers are aware that the vaccine is useful for protecting them and their unborn child
That injection we were taught that it helps prevent tetanus and when a mother is pregnant, the foetus gets immunity against tetanus because of the injection given to the mother. Expectant mother FGD 3
I had been told it protects both the mother and the child, but it did not affect me. Expectant mother FGD 1
Healthcare workers agree with the mothers, that they are aware that they should receive a vaccine. Sometimes, the mothers themselves can inquire why their counterparts were receiving the vaccine and not them. As per the Kenya Expended Programme for Immunization schedule, mothers are supposed to get the vaccine according to their number of pregnancies. What the mothers aren’t aware of is the importance of receiving the vaccine.
I could say that most mothers know they are supposed to get immunisation when expectant … Knowledge is low in terms of knowing like what the vaccine does, why they are being immunised and what it entails. There is a gap there, but they know they are supposed to come to the clinic. They know that when they come, they’re supposed to get a vaccination for tetanus and several jabs. Key informant 01
Of all the participants interviewed, 26% (27/104) reported that they knew people in their community who had ever refused a vaccine when expectant and 8% (8/104) had ever heard of negative information about vaccines in the recent past.
Some of the reasons for vaccine refusal include rumours in the community that the tetanus vaccine is for family planning.
You hear people say that they are for family planning; people say that they reduce your fertility. Expectant Mother FGD4
There are also instances where expectant mothers fail to receive the vaccine due to home deliveries.
There is a neighbour who was expectant from home … For all the nine months she has been home … She even delivered at home recently. Expectant Mother FGD2
The other one is my sister you tell her to go to clinic, and she tells you I am okay, no need for me to go to clinic, I will deliver at home, is it a must I go to hospital? Expectant mother FGD 1
There are those who give birth at the hospital but there are others who are afraid like me, I have given birth three times at home but then I have been told that I must give birth at the hospital Expectant mother FGD 4
These home deliveries are facilitated mostly by midwives or traditional birth attendants
Then there are the midwives they have a habit of asking you to visit them so that they can check the child’s progress, Expectant mother FGD2
I once carried my pregnancy to the end, from the first to the ninth month and never visited the clinic even once. I did not come for clinic not even a single day. I was going to these midwives who massaged me and told me my baby was okay, Expectant mother FGD 4
There were also concerns about women receiving an HIV test during their ANC visits.
Getting tested (for HIV) is why they fear coming to clinic … Because when you come, you cannot get services until your HIV status is known. Expectant Mother FGD1
The respondents also adduced religious reasons. Within our setting, participants reported that people from particular religious groups do not subscribe to vaccine uptake when expectant or even for their children.
There are those who don’t come to the clinic at all and they have other reasons like religion … There is a church that doesn’t believe in hospital and its services … They say God will help … They conceive and get to delivering without any vaccinations … God keeps them safe … They exist, but there are not so many; others are in that sect but still come for clinic … But those who hold on to that faith don’t come totally. Key informant 002
The decision on whether a young mother will seek vaccination is partly informed by the advice she will receive from decision-makers in the homestead. At least within our settings, a mother-in-law or older woman has a role in influencing health care services including vaccination.
There are those old women, our grandmothers, who in their time did not go to the hospital or anywhere when they became expectant; even in delivery, they got assistance from village Traditional Birth Attendants (TBAs) so as a daughter-in-law when you marry into that home, it is not easy to convince this woman to go to the hospital because they say I gave birth to your husband and I did not go to the hospital and I gave birth without any issues and right now he has grown without any problems, he is okay till now he has married you, so don’t stress yourself, just stay here I will look after you or a friend of mine will look after you. Expectant Mother FGD1
We asked participants to rank from a list of healthcare workers, family or other relatives, radio/TV and friends, which are their most trusted sources of information about vaccines for expectant mothers. We found that 77% (80/104) of participants used healthcare workers as their source of information about vaccines for expectant mothers. Most participants, 84% (87/104) ranked healthcare workers as their most trusted source of information, with 34% (35/104) ranking their friends as the least they could consult on information about maternal vaccines.
As the healthcare workers are the frontline government service providers, we tested the level of trust in the government and whether participants thought vaccines should be compulsory. Approximately 77% (80/104) and 20% (21/104) of the participants strongly agree or agree, respectively, that they trust that the government is deciding in their best interest with regard to vaccines for expectant mothers. In contrast, 53% (55/104) and 23% (24/104) of the participants strongly agree or agree, respectively, that vaccines for expectant mothers should be made compulsory.
Among the key informants, one reason maternal vaccine uptake is low is vaccine stockout, which affects vaccine delivery.
At times we get stock outs … yes as much as they (expectant mothers) would wish to get the vaccine by the time they come the vaccine is not there. Key informant 4
Frequent stock outs so they will tell you every time we come, there are stock outs so better we remain at home, Key informant 5
The attitude of the healthcare worker also plays a role on whether a mother will come back to take the vaccine or even visit the antenatal clinic.
Another thing which will make these mothers not to come is the attitude of the health provider at the facility. If a mother comes every day and am like you are shouting at me you are not giving me attention, it is like I tell you are not listening to me you are so arrogant I will not come back, I would rather stay at home. Key informant 6
Healthcare workload was noted as affecting vaccine delivery, especially in the lower-level health facilities where the healthcare worker’s main responsibility is to administer vaccines and offer other ANC services.
Only one nurse runs majority of our dispensaries and only one staff … running a facility you are the one giving immunizations, you are the one taking care of the pregnancy, you are the one taking care of the sick ones who are coming in, so it is actually hectic and by the end of the day they also need to rest … come at night, they cannot work day and night, at night they are home … and over the weekends again they are taking their offs. Key informant 5
We need more nurses. Currently in this Maternal Child Health (MCH) clinic, you can see this room is closed - it’s supposed to provide postnatal care, cervical cancer screening, and family planning services. But because we’re understaffed, we’ve had to close it. Now just one nurse must provide all these services in a single room, which forces clients to wait extremely long hours. This situation ultimately discourages mothers from returning to the clinic. Key informant 2
Then another thing we should add our manpower because me as nurse X I cannot say I know this and this and it’s me only every day, Key Informant 4
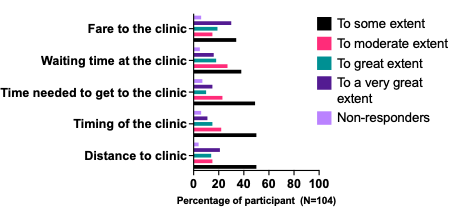
Since 2013, the Kenyan government has introduced two policies to reduce maternal and neonatal deaths: the abolition of client user fees and the provision of free maternity services in public health facilities (Pyone, Smith, and Van Den Broek 2017). We, therefore, tested to what extent other factors such as cost in terms of fare to the clinic, waiting time at the clinic, the time needed to get to the clinic, the timing of the clinic and distance to the clinic prevented expectant mothers from going to get the vaccine. In all instances, these factors affected vaccine uptake only to some extent ( Figure 2).
It is well-accepted that maternal vaccination significantly reduces neonatal morbidity and mortality (Blencowe et al. 2010). However, a growing number of people perceive vaccines as unsafe and unnecessary (Omer et al. 2009). In this study, we sought to understand factors that influence maternal vaccine uptake. We report results from the contextual influences and individual/social group influences.
Almost everyone reported general knowledge of the existence of vaccines. However, few knew how the tetanus toxoid maternal vaccine works and why it is administered to mothers. The lack of knowledge can be partly explained by the low education levels of our study participants; most of them had primary-level education. It is important to note that participants generally agreed that the tetanus vaccine was good for the mothers. Several factors limited maternal vaccine uptake. Rumours and misinformation around the tetanus vaccine within the community caused fears among expectant mothers. It was perceived that the tetanus vaccine was a family planning method, a message reinformed when the Kenyan government rolled out a tetanus vaccination campaign targeting school-going girls (WHO 2025). The fact that boys were excluded from the campaign made the community suspicious that the vaccine was to control fertility among young women. According to the 2029 Kenya Census (KNBS 2019) majority of Kenyans identify themselves with a particular religion. Indeed, in this study, almost all of the participants were Christians. We found that particular religious groups or sects were against modern medicine and particularly advised their congregants against using family planning methods. Additionally, they made those who heard the rumours about tetanus vaccine as a form of birth control to avoid going for the vaccine. It is worth noting that the government, through the Public Health Department, has put in place mechanisms to trace those missing out on vaccination and sometimes using community lead interventions to encourage vaccine uptake (Jain et al. 2024).
Although there has been concerted efforts by the Kenyan government to increase hospital access by rural mothers, a study conducted by Moindi et al., exploring risk perceptions associated with home deliveries estimated that approximately 26% of mothers in Kilifi County delivered at home (Moindi et al. 2016). We found that Traditional Birth Attendants (TBAs) and midwives remained important because mothers could access them easily and faster, especially if the dispensaries were far. Some mothers only sought the services of these TBAs throughout their pregnancy and, as a result, miss out on vaccinations. Within our setting, healthcare-seeking behaviours are partly influenced by older women within the homestead. We found that if these older women did not go to ANC clinics, they tended to discourage young mothers married to their sons from attending the clinic for vaccines when expectant.
Global trends indicate that healthcare workers remain the most trusted sources of information on health matters. In this study, the majority of the participants said they could consult healthcare workers on information related to vaccines. Very few people searched the internet if they had issues with vaccines. Considering this is a predominantly rural population, the cost of internet and smartphones could be a limiting factor.
Health system factors such as vaccine stockout were also identified by the key informants as a challenge to vaccine delivery. As much as the healthcare workers would like to maintain a high vaccine coverage, issues such as delays in vaccine delivery to the health facilities meant that even when mothers showed up and demanded vaccination, the vaccines were out of stock, causing a missed opportunity. Similar to what has been found in Ethiopia (Gebremichael et al. 2018), Tanzania (Maluka et al. 2020) and Uganda (Kajungu et al. 2020), we observed that if a healthcare worker was harsh, abusive or rude, it could discourage women from attending ANC clinics, which has a ripple effect on the uptake of vaccines by the mothers.
Most of our study populations were drawn from rural areas, including rural towns. It has been shown that rural areas tend to have lower education and health literacy (Das et al. 2017), factors important for vaccine uptake (Lorini et al. 2018). Therefore, our findings need to be interpreted within the context in which the study was done. Future studies are required to explore in-depth maternal vaccine hesitancy issues in urban areas in which the population have varying education levels and socioeconomic status.
Our study highlights factors that contribute to low maternal vaccine uptake. Continuous community engagement is required to address the fears, misconceptions, and rumours around tetanus vaccine uptake, which is important for laying the ground for future vaccine rollout for expectant mothers.
| Views | Downloads | |
|---|---|---|
| F1000Research | - | - |
|
PubMed Central
Data from PMC are received and updated monthly.
|
- | - |
Provide sufficient details of any financial or non-financial competing interests to enable users to assess whether your comments might lead a reasonable person to question your impartiality. Consider the following examples, but note that this is not an exhaustive list:
Sign up for content alerts and receive a weekly or monthly email with all newly published articles
Already registered? Sign in
The email address should be the one you originally registered with F1000.
You registered with F1000 via Google, so we cannot reset your password.
To sign in, please click here.
If you still need help with your Google account password, please click here.
You registered with F1000 via Facebook, so we cannot reset your password.
To sign in, please click here.
If you still need help with your Facebook account password, please click here.
If your email address is registered with us, we will email you instructions to reset your password.
If you think you should have received this email but it has not arrived, please check your spam filters and/or contact for further assistance.
{kind=link}
Response: We thank the reviewer for bringing this crucial update to our attention. We will rephrase the statement to read: The Kenya Expanded Programme on Immunization recommends that expectant women receive tetanus-diphtheria (Td) vaccine.
“Several factors that contribute to vaccine hesitancy have been reported. These include expectant women’s levels of knowledge and attitude towards the safety and efficacy of the vaccine (Bushar et al. 2017; Eppes et al. 2013), how the healthcare worker interacts with mothers (Bukenya and Freeman 1991)” – You may wish to revisit the paper cited here as it refers to missed opportunities for immunization (MOI) which is influenced by factors beyond hesitancy. For example, it is unclear how vaccine logistical issues, which contributes to MOI will affect hesitancy.
Response: We have revised the statement with a correct citation
These include expectant women’s levels of knowledge and attitude towards the safety and efficacy of the vaccine (Bushar et al. 2017; Eppes et al. 2013), how the healthcare worker interacts with mothers (R. J. Wilson et al. 2015)…
In the introduction section of the paper, it will be useful to provide and/or cite literatures on the importance and influence on immunization uptake by males, especially the heads of the households. This will allow for a better understanding of why males were also interviewed
Response: We will add the following paragraph to the introduction
Other factors that influence motivation for maternal vaccine uptake include the views of the people around the expectant women. It has been shown that husbands and mothers-in-law play a role in the expectant women's decision-making process during pregnancy, including whether to take or not take a vaccine, coupled with the fact of the woman’s limited autonomy within the family setting, especially so within the African context (Johm et al. 2021). In other settings, expectant women seek advice on whether to be vaccinated or not from their female family members such as sisters who already have children, mothers and aunts but less so from their male partners (R. Wilson, Paterson, and Larson 2019)
Methods – Study populations
It will be useful to give a bit of an insight into the random sampling method of the expectant women attending ANC and men and women of reproductive age at the community level in four different locations/wards
Response: We thank the reviewer for pointing this out and apologize for any confusion this statement might have caused. We will revise to ensure consistency throughout the text.
We used convenient sampling for expectant women attending the ANC clinic at select participating health care facilities of Kilifi County Hospital (KCH), Mnarani and Ngeranya dispensaries. We identified women and men of reproductive age at the community level through the assistance of Community Health Extension Officers, who have good knowledge of their communities and also served as study facilitators. Other studies have also used this approach (Watson-Jones et al. 2015).
Any reason why the coverage of the first dose of TT was used rather than at least two doses (TT2+)? One dose TT is not known to confer any level of immunity against tetanus, while a child born to a mother who receives at least two well-spaced doses is considered to be protected at birth (PAB) against tetanus.
Response: In general, in Kenya, tetanus-diphtheria (Td) vaccine uptake remains low (Otieno et al. 2021, 2017–2018). We used the first dose of vaccine as indicative of coverage to guide us to select study sites and not to directly link it to immunity accorded by the vaccine per se.
Methods – data collection
How many FGDs were conducted?
Response: Our study used the triangulation method to understand factors contributing to maternal vaccine uptake within the rural setting of Kilifi, Kenya. We conducted four focus group discussions with expectant women. The FGDs took place at the participating health care centers. Furthermore key informant interviews and survey questionnaires were also used to help us understand the contextual factors for maternal vaccine uptake.
Results
General vaccination knowledge and awareness
It will be useful to disaggregate this data by sex, to assess the knowledge about maternal immunization between males and females.
Response: We thank the reviewer for this comment. We will insert a table breakdown of the responses by sex, below is those who responded yes to the general vaccination knowledge and awareness.
Question
Males N (%)
Females N(%)
Have you ever heard of a vaccine?
38 (95)
63 (100)
Do you know which vaccine women get when expectant?
22 (55)
50 (79.4)
Have you ever heard of tetanus vaccine
36 (93.2)
60 (95.2)
Discussion
“Rumors and misinformation around the tetanus vaccine within the community caused fears among expectant mothers. It was perceived that the tetanus vaccine was a family planning method, a message reinformed when the Kenyan government rolled out a tetanus vaccination campaign among school-going girls. The fact that boys were excluded from the campaign made the community suspicious that the vaccine was to control fertility among young women” - It will be useful to know if the same perception holds for tetanus vaccines given through the routine immunization system, during ANC visits. The delivery of tetanus and diphtheria toxoid-containing vaccines along life-course: 3 primary series of DTP during infancy, 1st booster dose at 2nd year of life, 2nd booster dose during school entry (4 - 7 years) and 3rd booster during early adolescence (9 - 15 years) does not have gender discrimination and may help to dispel the existing rumor
Response: We thank the reviewer for this comment. We agree that rolling out the DTP life course vaccine to both girls and boys may perhaps dispel the rumours. Future studies will be needed to monitor community perceptions as the vaccine is rolled out and careful risk communication strategies implemented.
References
Johm, Penda, Nicole Nkoum, Amie Ceesay, El Hadji Mbaye, Heidi Larson, and Beate Kampmann. 2021. ‘Factors Influencing Acceptance of Vaccination during Pregnancy in The Gambia and Senegal’. Vaccine 39 (29): 3926–34. https://doi.org/10.1016/j.vaccine.2021.05.068.
Otieno, Nancy A., Fauzia A. Malik, Stacy W. Nganga, Winnie N. Wairimu, Dominic O. Ouma, Godfrey M. Bigogo, Sandra S. Chaves, et al. 2021. ‘Decision-Making Process for Introduction of Maternal Vaccines in Kenya, 2017–2018’. Implementation Science 16 (1): 39. https://doi.org/10.1186/s13012-021-01101-7.
Watson-Jones, Deborah, Nelly Mugo, Shelley Lees, Muthoni Mathai, Sophie Vusha, Gathari Ndirangu, and David A. Ross. 2015. ‘Access and Attitudes to HPV Vaccination amongst Hard-To-Reach Populations in Kenya’. PLoS ONE 10 (6): e0123701. https://doi.org/10.1371/journal.pone.0123701.
Wilson, R., P. Paterson, and H. J. Larson. 2019. ‘Strategies to Improve Maternal Vaccination Acceptance’. BMC Public Health 19 (1): 342. https://doi.org/10.1186/s12889-019-6655-y.
Wilson, Rose J., Pauline Paterson, Caitlin Jarrett, and Heidi J. Larson. 2015. ‘Understanding Factors Influencing Vaccination Acceptance during Pregnancy Globally: A Literature Review’. Vaccine, Advancing Maternal Immunization Programs through Research in Low and Medium Income Countries, 33 (47): 6420–29. https://doi.org/10.1016/j.vaccine.2015.08.046.
Response: We thank the reviewer for bringing this crucial update to our attention. We will rephrase the statement to read: The Kenya Expanded Programme on Immunization recommends that expectant women receive tetanus-diphtheria (Td) vaccine.
“Several factors that contribute to vaccine hesitancy have been reported. These include expectant women’s levels of knowledge and attitude towards the safety and efficacy of the vaccine (Bushar et al. 2017; Eppes et al. 2013), how the healthcare worker interacts with mothers (Bukenya and Freeman 1991)” – You may wish to revisit the paper cited here as it refers to missed opportunities for immunization (MOI) which is influenced by factors beyond hesitancy. For example, it is unclear how vaccine logistical issues, which contributes to MOI will affect hesitancy.
Response: We have revised the statement with a correct citation
These include expectant women’s levels of knowledge and attitude towards the safety and efficacy of the vaccine (Bushar et al. 2017; Eppes et al. 2013), how the healthcare worker interacts with mothers (R. J. Wilson et al. 2015)…
In the introduction section of the paper, it will be useful to provide and/or cite literatures on the importance and influence on immunization uptake by males, especially the heads of the households. This will allow for a better understanding of why males were also interviewed
Response: We will add the following paragraph to the introduction
Other factors that influence motivation for maternal vaccine uptake include the views of the people around the expectant women. It has been shown that husbands and mothers-in-law play a role in the expectant women's decision-making process during pregnancy, including whether to take or not take a vaccine, coupled with the fact of the woman’s limited autonomy within the family setting, especially so within the African context (Johm et al. 2021). In other settings, expectant women seek advice on whether to be vaccinated or not from their female family members such as sisters who already have children, mothers and aunts but less so from their male partners (R. Wilson, Paterson, and Larson 2019)
Methods – Study populations
It will be useful to give a bit of an insight into the random sampling method of the expectant women attending ANC and men and women of reproductive age at the community level in four different locations/wards
Response: We thank the reviewer for pointing this out and apologize for any confusion this statement might have caused. We will revise to ensure consistency throughout the text.
We used convenient sampling for expectant women attending the ANC clinic at select participating health care facilities of Kilifi County Hospital (KCH), Mnarani and Ngeranya dispensaries. We identified women and men of reproductive age at the community level through the assistance of Community Health Extension Officers, who have good knowledge of their communities and also served as study facilitators. Other studies have also used this approach (Watson-Jones et al. 2015).
Any reason why the coverage of the first dose of TT was used rather than at least two doses (TT2+)? One dose TT is not known to confer any level of immunity against tetanus, while a child born to a mother who receives at least two well-spaced doses is considered to be protected at birth (PAB) against tetanus.
Response: In general, in Kenya, tetanus-diphtheria (Td) vaccine uptake remains low (Otieno et al. 2021, 2017–2018). We used the first dose of vaccine as indicative of coverage to guide us to select study sites and not to directly link it to immunity accorded by the vaccine per se.
Methods – data collection
How many FGDs were conducted?
Response: Our study used the triangulation method to understand factors contributing to maternal vaccine uptake within the rural setting of Kilifi, Kenya. We conducted four focus group discussions with expectant women. The FGDs took place at the participating health care centers. Furthermore key informant interviews and survey questionnaires were also used to help us understand the contextual factors for maternal vaccine uptake.
Results
General vaccination knowledge and awareness
It will be useful to disaggregate this data by sex, to assess the knowledge about maternal immunization between males and females.
Response: We thank the reviewer for this comment. We will insert a table breakdown of the responses by sex, below is those who responded yes to the general vaccination knowledge and awareness.
Question
Males N (%)
Females N(%)
Have you ever heard of a vaccine?
38 (95)
63 (100)
Do you know which vaccine women get when expectant?
22 (55)
50 (79.4)
Have you ever heard of tetanus vaccine
36 (93.2)
60 (95.2)
Discussion
“Rumors and misinformation around the tetanus vaccine within the community caused fears among expectant mothers. It was perceived that the tetanus vaccine was a family planning method, a message reinformed when the Kenyan government rolled out a tetanus vaccination campaign among school-going girls. The fact that boys were excluded from the campaign made the community suspicious that the vaccine was to control fertility among young women” - It will be useful to know if the same perception holds for tetanus vaccines given through the routine immunization system, during ANC visits. The delivery of tetanus and diphtheria toxoid-containing vaccines along life-course: 3 primary series of DTP during infancy, 1st booster dose at 2nd year of life, 2nd booster dose during school entry (4 - 7 years) and 3rd booster during early adolescence (9 - 15 years) does not have gender discrimination and may help to dispel the existing rumor
Response: We thank the reviewer for this comment. We agree that rolling out the DTP life course vaccine to both girls and boys may perhaps dispel the rumours. Future studies will be needed to monitor community perceptions as the vaccine is rolled out and careful risk communication strategies implemented.
References
Johm, Penda, Nicole Nkoum, Amie Ceesay, El Hadji Mbaye, Heidi Larson, and Beate Kampmann. 2021. ‘Factors Influencing Acceptance of Vaccination during Pregnancy in The Gambia and Senegal’. Vaccine 39 (29): 3926–34. https://doi.org/10.1016/j.vaccine.2021.05.068.
Otieno, Nancy A., Fauzia A. Malik, Stacy W. Nganga, Winnie N. Wairimu, Dominic O. Ouma, Godfrey M. Bigogo, Sandra S. Chaves, et al. 2021. ‘Decision-Making Process for Introduction of Maternal Vaccines in Kenya, 2017–2018’. Implementation Science 16 (1): 39. https://doi.org/10.1186/s13012-021-01101-7.
Watson-Jones, Deborah, Nelly Mugo, Shelley Lees, Muthoni Mathai, Sophie Vusha, Gathari Ndirangu, and David A. Ross. 2015. ‘Access and Attitudes to HPV Vaccination amongst Hard-To-Reach Populations in Kenya’. PLoS ONE 10 (6): e0123701. https://doi.org/10.1371/journal.pone.0123701.
Wilson, R., P. Paterson, and H. J. Larson. 2019. ‘Strategies to Improve Maternal Vaccination Acceptance’. BMC Public Health 19 (1): 342. https://doi.org/10.1186/s12889-019-6655-y.
Wilson, Rose J., Pauline Paterson, Caitlin Jarrett, and Heidi J. Larson. 2015. ‘Understanding Factors Influencing Vaccination Acceptance during Pregnancy Globally: A Literature Review’. Vaccine, Advancing Maternal Immunization Programs through Research in Low and Medium Income Countries, 33 (47): 6420–29. https://doi.org/10.1016/j.vaccine.2015.08.046.